|
 |
|

July / August 2005
Medication Safety
Averting Highest-Risk Errors Is First Priority
Part II: Nursing Satisfaction,Wireless Networking,"Smart"Pain Management, Best Practice Improvements, and ROI
Tim Vanderveen, PharmD, MS
Targeting medication safety efforts to give first priority to averting the highest-risk errors allows hospitals to achieve the most rapid and significant impact on improving medication safety. This series of articles describes technology advances that provide new tools and data to help clinicians, administrators, and risk managers avert the medication errors associated with the highest risk of harm — intravenous (IV) medication errors (Wilson & Sullivan, 2004; Williams & Maddox, 2005).
Part I in this series (May/June issue, PSQH) reviewed the need for improved IV medication safety; comparative risk of IV vs. oral medications; the "speed to impact" (costs, time, ease of implementation, and capabilities to prevent high-risk medication errors) of various medication safety technologies; development of "smart" infusion systems; and published results to date.
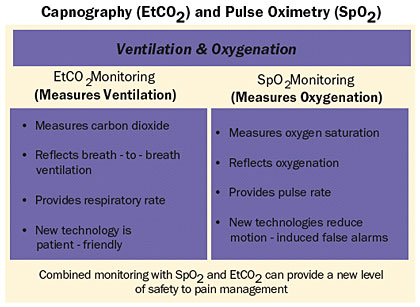
This article reviews nursing satisfaction and recent advances, including wireless networking, "smart" patient-controlled analgesia (PCA) with continuous respiratory monitoring, best practice improvements, and return on investment (ROI).
Nursing Satisfaction
Experience has shown that nursing acceptance is critical to the successful implementation and use of new technology. Nursing administrators at St. Joseph's/Candler Health System, a 675-bed facility in Savannah, Georgia, believe that positive feedback regarding the IV medication safety systema resulted from the level of pre-implementation education of nursing and hospital staff coupled with the involvement of nursing in research and implementation of the technology. CQI data and regular checks using direct observation show 98% to 100% compliance for nurses using the safety software for programming. Implementation of the system was felt to demonstrate the hospital's commitment to nurses and to give SJCHS an edge in nursing retention and recruitment (Fields & Peterman, 2005).
A survey conducted at The Nebraska Medical Center (680 beds) shows that over 90% of users said the IV safety system was "Easy" or "Somewhat Easy" to program and would "Agree" or "Strongly Agree" that the system provides a valuable safety net at the point of care (Graham, 2004). Results show that nurses strongly prefer using the infusion safety system over their previous IV pumps. Data also showed that use of the safety software prevented potentially fatal medication errors (Graham, 2004; Malashock, et al., 2004). Staff feels that infusion safety technology is needed to protect both patients and nurses against critical errors at the point of care (Graham, 2004).
Staff at City of Hope, one of the top 100 cancer centers, had a similar response. Nursing administrators felt that implementation of the IV safety system and the resulting CQI data on averted errors allowed cultural change to be introduced in incremental steps, as nurses saw the impact of this technology on medication errors (Steingass 2004).
Best Practice Improvements
The examples below are representative of best practice improvements that have been made as a result of infusion safety system implementation.
Sedation Use. During beta testing at Vanderbilt University Medical Center (631 beds), nurses reported that trauma patients transferred from the ICU often required a prolonged period to become responsive enough to start rehabilitative therapy.�As a result of smart system CQI data analysis, "titrate to sedation" was replaced by titration to a specific scale. Staff education focused on using the scale to more closely monitor patient response.�After implementation of these changes, reports from nurses indicated decreased time between transfer and start of therapy, leading to decreased patient recovery time, decreased length of stay, and decreased potential for sedation-related complications (Hatcher, et al., 2004; Thurman, et al., 2004).
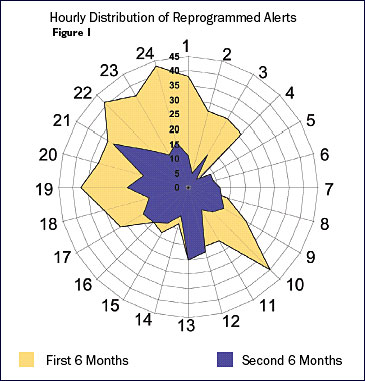
Staffing Effectiveness. At Children's Hospital of San Diego, chronogram analysis (Figure 1) led to highly targeted practice improvement initiatives to address peak times for medication errors. Units were closed during shift change, and the timing of several elective activities was changed to reduce distractions. Since these changes, pump alerts are much less frequent and all of the former error peaks have been eliminated (Billman, 2004).
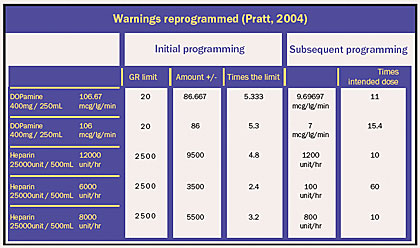
Improved Medication Protocol. Using CQI data from the safety software, staff at St. Joseph's/Candler revised the heparin protocol to eliminate rate calculations by programming the dose (units/kg/hour) directly into the smart pump. This eliminated at least three steps in the medication process, multiple calculations, and multiple opportunities for error, thereby improving the safety and timeliness of heparin administration. The system allowed staff to discover that, if IV drug labels were reformulated to include the total volume and amount of drug, nursing staff would be able to program the system more easily and deliver the correct dose of medication (Williams & Maddox, 2005).
Return On Investment (ROI)
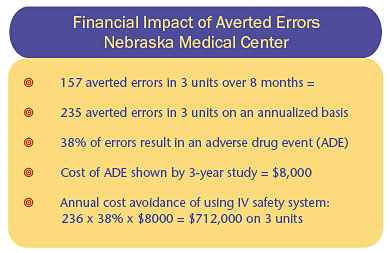
Analysis of reprogramming events documented in CQI logs at The Nebraska Medical Center for three nursing units involved in an 8-month study showed that an annual incremental expense that was avoided through use of the IV safety systems would be approximately $712,000 (Table 1) (Graham, 2004).
|
|
|
 |










|
 |