Using Information From External Errors to Signal a “Clear and Present Danger”
A system cannot understand itself, regardless of the number and quality of investigations and root cause analyses conducted on internal errors. Quality guru Dr. W. Edwards Deming summarized this phenomenon by noting that organizations with an internal focus “may learn a lot about ice, yet know very little about water” (Deming, 1994).
This concept is applicable to learning from your internal errors, too. Seeking outside knowledge from the literature or experts in the field when reviewing your own errors can open your eyes to vulnerabilities that are hard to see within the processes you have built or work in every day. Even including staff from a different department when reviewing errors can be an eye-opening experience. Knowledge from the outside is necessary and provides us with a lens to examine what we are doing, suggestions for what we might do differently, and a roadmap for improvement (Conway, 2008).
External resources also provide us with a wealth of information that can be used to make the safest decisions when providing patient care. When we stand at a fork in the road and are unsure where each one leads, it would be foolish to choose whichever “seems” best without looking at information easily within our reach from others who have already traveled each road.
The Centers for Medicare & Medicaid Services (CMS) agrees. In its Interpretive Guidelines for Hospitals (§482.25 [a]), Condition of Participation: Pharmaceutical Services, CMS requires hospitals to take steps to prevent, identify, and minimize medication errors, and for hospital pharmacies to “be aware of external alerts to real or potential pharmacy-related problems in hospitals.”
Overcoming biases to allow learning
To best promote patient safety, it is crucial to seek out information about external errors, to hold on to your initial feelings of surprise and uncertainty when you read about these errors, and to resist the temptation to gloss over what happened or attribute the problem to an individual different than you (Weick & Sutcliffe, 2001). It is in the brief interval between the initial unease when reading about an external error and the normalization of error—convincing yourself that it couldn’t happen to you—that significant learning can occur. For that reason, ISMP highly recommends sharing sto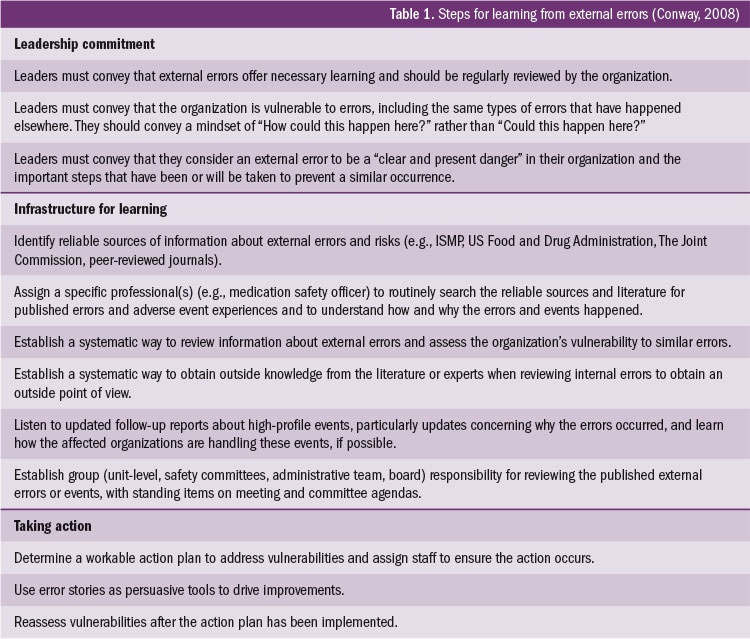 ries of external errors with staff, such as those published in the ISMP Medication Safety Alert! and summarized each quarter in the ISMP Quarterly Action Agenda (www.ismp.org/sc?id=2865).
ries of external errors with staff, such as those published in the ISMP Medication Safety Alert! and summarized each quarter in the ISMP Quarterly Action Agenda (www.ismp.org/sc?id=2865).
The ISMP Quarterly Action Agenda was initiated 19 years ago for the purpose of encouraging organizations to use information about safety problems and errors that have happened in other organizations to prevent similar problems or errors in their practice sites. The Agenda is prepared for an interdisciplinary committee to stimulate discussion and action to reduce the risk of medication errors. Each item in the Agenda includes a brief description of the medication safety problem, a few recommendations to reduce the risk of errors, and the issue number to locate additional information. The Agenda is also available in a Microsoft Word format that allows organizational documentation of an assessment, actions required, and assignments for each agenda item. The latest Quarterly Action Agenda was published in the January 26, 2017, newsletter and will continue to be published every quarter in the January, April, July, and October issues.
Additional steps organizations should take to establish a system for ongoing risk identification and learning from external errors can be found in Table 1.