ISMP: Patient-Controlled Analgesia
July/August 2013
![]()
ISMP
Patient-Controlled Analgesia
Fatal PCA adverse events continue to happen… Better patient monitoring is essential to prevent harm.
A patient underwent surgical repair of a heel injury. Within 15 minutes of arrival in the postanesthesia care unit (PACU), he received IV doses of meperidine 75 mg, morphine 4 mg, and fentaNYL 25 mcg for pain. The patient’s surgeon also ordered “PCA per anesthesia.” A nurse anesthetist wrote an order for morphine patient-controlled analgesia (PCA) 1 mg/mL, 3 mg per demand dose, lock out of 10 minutes, and a basal rate of 1 mg/hour. Although the patient was obese and anxious about inadequate pain control, the prescribed demand dose—potentially adding up to 18 mg/hour—along with a basal infusion were too much for the patient given his opioid naïve status. In fact, based on morphine prescribing information, the dose might have been high even for an opioid tolerant patient.
A pharmacist reviewed the PCA order but did not investigate the patient’s current opioid usage. He did not question the 3 mg demand dose or the basal infusion, neither of which is recommended for an opioid naïve patient. The morphine PCA was started around 8 pm while the patient was in the PACU. The patient had not received preoperative PCA instructions, so the PACU nurse taught the patient to self-administer the doses. No further education was provided, and the patient’s family was not warned about the hazards of anyone other than the patient administering a dose.
Within 30 minutes of starting the PCA, the patient had given himself 3 doses of morphine, 3 mg each. He reported that his pain was “receding,” but a pain score was not documented. Over the next 5 hours, the patient administered 17 more doses for a total of 20 doses (60 mg), and the basal infusion delivered an additional 5.5 mg of morphine. Most of the doses were administered between 8 pm and midnight. It’s unknown if the patient’s wife, who remained at the patient’s bedside until midnight, periodically awakened the patient and encouraged him to administer a dose or if she administered doses for him while he slept. Around 2 am, the patient was found in respiratory arrest. Resuscitation efforts were unsuccessful.
Since PCA initiation, nurses had been monitoring the patient every 30 minutes for the first hour, every hour for the next 3 hours, then every 2 hours. However, monitoring was less frequent than required by hospital policy and less often than typically recommended for patients receiving PCA (San Diego Patient Safety Council, 2009). In addition, the assessment of pain was infrequent, and the assessment of respiratory status did not include the depth, pattern, effort of respirations, and breath sounds. Pulse oximetry was not used to measure oxygen saturation, although policy required its use and the oximetry equipment was available in the patient’s room.
Further, a standard sedation assessment scale was not utilized. Progressive signs of impending respiratory arrest were not recognized, particularly those related to the patient’s level of sedation. After the first hour of PCA use, the patient was assessed as “awake and alert” with a pain assessment score of 4 (scale 1-10). As the evening went on, the patient became “sleepy and drowsy but easily aroused,” although no pain assessment was documented. By midnight, 4 hours after starting the PCA, the patient was “sleeping and snoring loudly,” and no attempts were made to arouse the patient to assess his level of sedation and pain. Two hours later, the patient was described as “sleeping and snoring loudly, but arousable” with no further details. Shortly thereafter, the patient was found in respiratory arrest.
One factor that probably contributed to the patient’s respiratory arrest is the delayed transfer of morphine across the blood-brain barrier (Lotsch et al., 2006; Lotsch et al., 2001). The repeated administration of relatively high doses of morphine at short intervals and the delayed transfer of the drug to the brain made it possible for the fatal event to occur almost 2 hours after the bulk of self-administered doses were taken. A patient with severe pain may tolerate larger doses of morphine because the pain helps counteract the respiratory-depressant effects of opioids (Lotsch et al., 2006; Borgbjerg et al., 1996; Grissinger, 2013). However, once the pain subsides, previously adequate breathing can quickly become inadequate with the onset of sedation or sleep (Borgbjerg et al., 1996; Grissinger, 2013).
Given the widespread use of PCA, most hospitals likely have a “PCA story” to tell (San Diego Patient Safety Council, 2009). Fortunately, not all of these stories have resulted in death. However, studies have documented the association of PCA with harmful and fatal errors (Lotsch et al., 2006; Hicks et al., 2008), and analyses of voluntary reports of events have shown a four-fold higher risk of harm with PCA errors than with other reported medication errors (San Diego Patient Safety Council, 2009). In most cases, characteristics that place patients at higher risk for opioid-induced respiratory depression have not been considered, and patient monitoring has been inadequate (Stoelting & Weinger, 2009; Weinger, 2006–2007).
Safe Practice Recommendations
ISMP has written about PCA errors numerous times (ISMP, 2003a; ISMP, 2003b), describing many of the causative factors, including prescribing errors, failing to determine the patient’s opioid tolerance and identify risk factors associated with respiratory depression, lack of educating patients and families about PCA, and inadequate monitoring. While many things went wrong in the event described above, the remainder of this article focuses on appropriate monitoring of patients receiving PCA—a critical, lifesaving activity that can provide an early warning of impending complications, thus preventing patient harm even in the presence of an error.
Along with a basic physical assessment and collection of vital signs, the following parameters are also important when monitoring patients receiving PCA.
Pain Assessment
The patient’s level of pain must be continually assessed during use of PCA to evaluate the treatment’s effectiveness. Use of a standard pain scale and/or tool (e.g., Wong-Baker Faces Scale) is highly recommended for accuracy and ease of eliciting a patient’s description of discomfort (San Diego Patient Safety Council, 2009). While the goal of PCA is pain relief, remember that pain relief can signal the loss of a compensatory mechanism that combats the respiratory-depressant effects of opioids. Thus, monitoring should be stepped up, and PCA doses may need to be reduced if pain relief is accompanied by oversedation.
Sedation Assessment
Sedation is an extremely useful assessment parameter to observe the clinical effects of opioids. In fact, sedation is the most important predictor of respiratory depression in patients receiving IV opioids—a fact that only 22% of physicians, pharmacists, and nurses knew when taking a recent opioid knowledge assessment (Grissinger, 2013). Sedation generally precedes significant respiratory depression. While pain can counteract opioid-induced respiratory depression, sleep can intensify the depressant effects. In addition, as carbon dioxide levels increase with respiratory depression, patients experience a reduced level of consciousness that is additive to the opioid sedative effects (San Diego Patient Safety Council, 2009).
Thus, for patients receiving PCA, early recognition of excessive sedation and intervention is essential.
A standard sedation scale should be used when assessing patients receiving PCA. The San Diego Patient Safety Council, which created a useful set of PCA guidelines for opioid naïve patients (San Diego Patient Safety Council, 2009), prefers the Richmond Agitation Sedation Scale (RASS; Ely et al., 2003) because it is simple to use and combines sedation and agitation into one scale. However, some hospitals use the Pasero, Ramsey, or Glasgow Coma scales.
To assess sedation, health professionals must evaluate how much stimulation is necessary to evoke the desired response from the patient; thus, one must first observe the patient. If the patient is awake, ask the patient a question and evaluate the response to determine if the patient is alert and oriented. If the patient is not alert (eyes closed), assess the patient’s response to verbal stimuli first. For example, the RASS scale (Ely et al., 2003) suggests stating the patient’s name and asking the patient to open his or her eyes and look at the speaker. The degree of movement and length of eye contact is evaluated to assess the sedation level. If the patient does not respond to verbal requests, physical stimulation is used, such as lightly shaking the patient’s shoulder to evaluate the response. Practitioners should have clear guidance regarding which levels of the sedation scale would indicate the need to increase the frequency of monitoring, adjust PCA doses, stop the PCA, call the prescriber, provide airway support and/or oxygen, and/or administer naloxone.
Respiratory Assessment
Respiratory assessments should include evaluation of the rate and quality of respirations. A respiratory rate of 10 breaths per minute or less should signal possible discontinuation of PCA (San Diego Patient Safety Council, 2009). The depth of respirations (i.e., normal, shallow, deep), pattern of respirations (i.e., regular, irregular), quality of respiratory effort (i.e., effortless, comfortable, labored), and breath sounds (i.e., clear, noisy, snoring, gurgling, stridor) are all important parameters when assessing respiration quality.
The Anesthesia Patient Safety Foundation (APSF) also recommends routine use of technology to continuously monitor ventilation in patients known to be at high risk for respiratory depression (e.g., preexisting respiratory impairment, sleep apnea, elderly or obese patients) and consideration of its use when possible for all patients receiving PCA (Stoelting & Weinger, 2009). Continuous pulse oximetry should be routine, although practitioners should be aware that oximetry readings may remain near normal for minutes after a patient stops breathing Weinger, 2006–2007). Thus, the APSF suggests using capnography whenever possible (even if intermittent) to detect unrecognized hypoventilation and carbon dioxide retention (Stoelting & Weinger, 2009). APSF also recommends limiting the use of supplemental oxygen when possible for patients receiving PCA, especially if pulse oximetry is the only technology used to detect hypoventilation. For patients receiving supplemental oxygen, there is no evidence that monitoring of oxygen saturation provides an additional measure of safety (McCarter et al., 2008).
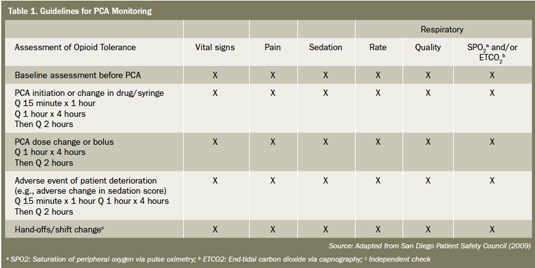
Frequency of Assessments
To be effective, patient monitoring must be conducted at the proper intervals. Guidelines that can be used to assess the adequacy of monitoring frequencies have been developed by the San Diego Patient Safety Council (see Table 1, page 44). Hospitals may want to monitor patients more frequently at night, as opioid-induced respiratory depression is more common between midnight and 6 a.m. (Borgbjerg et al., 1996). Please keep in mind that the purpose and frequency of monitoring should be explained to patients and their families so they understand and expect to be awakened and monitored frequently.
Click here to view a larger version in a separate window.
This column was prepared by the Institute for Safe Medication Practices (ISMP), an independent, nonprofit charitable organization dedicated entirely to medication error prevention and safe medication use. Any reports described in this column were received through the ISMP Medication Errors Reporting Program. Errors, close calls, or hazardous conditions may be reported online at www.ismp.org or by calling 800-FAIL-SAFE (800-324-5723). ISMP is a federally certified patient safety organization (PSO), providing legal protection and confidentiality for patient safety data and error reports it receives. Visit www.ismp.org for more information on ISMP’s medication safety newsletters and other risk reduction tools. This article appeared originally in the May 30, 2013, issue of the ISMP Medication Safety Alert!
References