Patient Engagement: How To Stay Connected In Healthcare
By Andrew Bonner
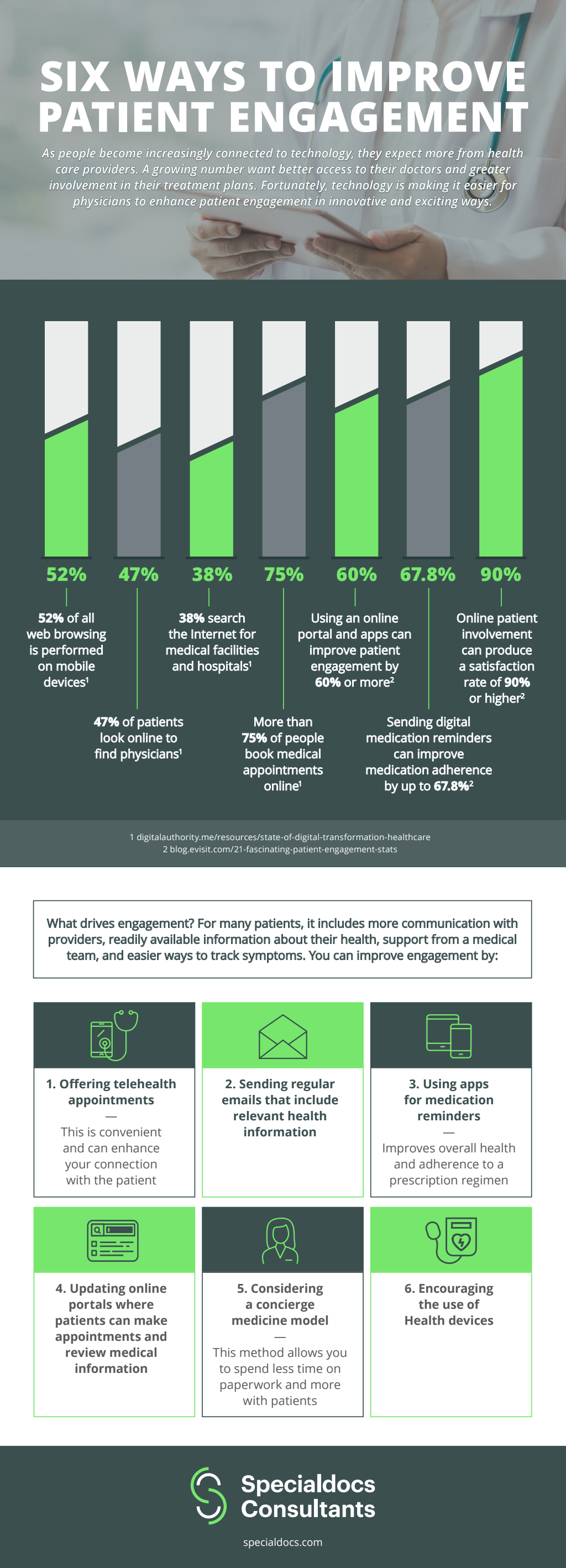
Strong patient engagement is more than convenience. It improves outcomes, strengthens trust, and ensures that care plans are followed effectively. Healthcare systems and providers are increasingly looking for ways to keep patients connected beyond the clinic visit, and technology is playing a major role in making that possible.
Digital tools for connection
Electronic health records with patient portals give individuals direct access to their medical information. Test results, prescriptions, and care instructions can be reviewed without waiting for phone calls or mailed letters. Secure messaging features also allow patients to send questions to providers quickly, reducing gaps in communication. Mobile apps add another layer, offering appointment reminders, educational resources, and even symptom trackers that help patients stay engaged between visits.
The role of telehealth
Telehealth has moved beyond urgent care visits. It is now being integrated into ongoing management of chronic conditions such as diabetes or hypertension. Regular virtual check-ins help providers monitor progress without requiring patients to travel, saving time and resources. For patients with mobility challenges or those living in rural areas, this type of engagement ensures that care remains consistent and accessible.
Personalized engagement strategies
Every patient interacts differently with healthcare. Some prefer digital tools, while others rely on direct phone calls or in-person visits. Providers are increasingly segmenting their approaches, identifying which communication channels best suit each patient group. For example, younger patients may be more responsive to app notifications, while older patients may benefit from scheduled phone outreach. Concierge medical services are also expanding, offering highly personalized engagement for patients who need or expect a more direct line of communication with their providers.
Building trust through transparency
Engagement is not only about tools but also about trust. Patients want clear explanations of test results, transparent discussions about treatment options, and consistent follow-up. Providers who prioritize open communication create stronger relationships, which increases adherence to care plans and reduces the likelihood of readmissions.
Healthcare will continue to rely on engagement strategies that blend technology with human connection. The goal is simple: make patients feel seen, heard, and supported. A well-connected patient is more likely to participate in their care, which benefits both the individual and the healthcare system as a whole. For more information, see the accompanying resource below.
Andrew Bonner is Director of Marketing at Specialdocs Consultants. Bonner has over 15 years of marketing experience in the healthcare industry. Prior to joining Specialdocs, he served as Marketing Director for two mid-sized physician groups, driving significant growth through successful lead acquisition, customer engagement and ad creation/placement strategies. Bonner is committed to improving the professional and personal lives of physicians ready to make the transition to the Specialdocs concierge model.