First, Protect the Patient from Harm
July / August 2010
First, Protect the Patient from Harm
Applying Adult Learning Principles to Patient Safety
“First, do no harm.”
Today, unlike in the time of Hippocrates, evidence of harm may not become immediately obvious during healthcare interventions. For example, a lapse in attention while inserting a central line may result in a blood stream infection that becomes apparent days later. A wrong site surgery may go unnoticed until after the effects of anesthesia subside. An incorrect dosage of medication may not be recognized until an adverse drug event occurs.
During the past decade, there has been no shortage of statistics showing the hazards awaiting those seeking healthcare services. As a consequence, hospitals have undertaken an abundance of initiatives to prevent harm among patients. Despite massive attempts to educate healthcare staff regarding patient safety measures, the Agency for Healthcare Research and Quality (AHRQ, 2007) reports patient safety is improving at a disappointing 1% per year.
Hospitals, anxious to meet accreditation standards, measure staff knowledge of the National Patient Safety Goals set forth by The Joint Commission since 2003. However, the AHRQ evidence suggests being knowledgeable of threats to patient safety is not sufficient to change the behavior in ways that are necessary to improve patient outcomes on a large scale. Higher levels of cognition are required by healthcare workers to comprehensively reduce medical error and effect culture change. To accomplish this, adult learning principles are coupled with higher levels of the cognitive domain and applied to patient safety situations in an effort to prevent error throughout the clinical setting. In other words healthcare workers learn how to first, protect the patient from harm.
Medical Errors in Healthcare
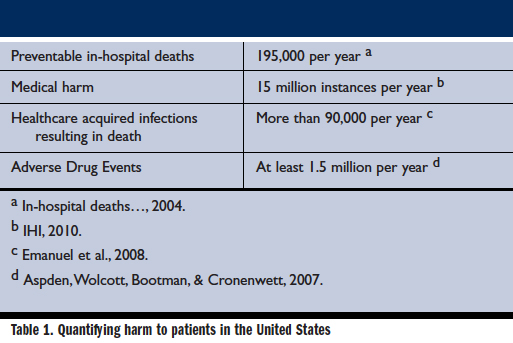
Medical errors have produced tragically high numbers of deaths and injuries to patients. An industry dedicated to protecting lives has become the eighth leading cause of death (Sexton, Thomas, & Helmreich, 2000; Vicente, 2002). As Table 1 shows, the magnitude of harm to human life is considerable. While most research has been performed in the in-patient setting, there is no reason to believe patient harm does not occur with disturbing frequency in other settings such as private practice, skilled nursing facilities, pharmacies, and ambulatory surgical centers. (Aspden, Wolcott, Bootman, & Cronenwett, 2007; WHO, 2007a).
Medical error has also become costly beyond human suffering and potential litigation. Medicare no longer pays hospitals for the treatment of many errors deemed preventable by regulatory agencies. As a result, attempts to eliminate harmful incidents, correct near misses, and identify unsafe conditions have assumed both clinical and administrative priority throughout healthcare.
Where did the good intentions of “First, do no harm” go wrong? Miraculous advancements in science during the past few decades have increased the complexity of our healthcare system. According to one observer in an AHRQ study of mistakes made in intensive care units, many errors occur because the knowledge base required to deliver safe care exceeds the storage capacity of the human brain (Quality Interagency Coordination Task Force, 2000). The sobering reality is that years of advances to save lives have created a system that sometimes unintentionally kills patients.
As advancements in diagnosis and treatment continue, we must teach healthcare workers first, to protect the patient from harm by managing the relentless change and multi-faceted complexity that threatens patient safety.
Defining Patient Safety
The Institute of Medicine defines patient safety as “freedom from accidental injury.” According to the Patient Safety Education Project (PSEP)(Emanuel et al., 2008), beyond this obvious definition lies “a highly contextual matter” covering a broad spectrum of concepts and environments.
The PSEP says the concern for patient safety occurs in microenvironments where patient and caregiver interactions happen, such as emergency departments, labor rooms, or cardiac catheterization labs. This is where the successes or failures of all systems to ensure safety converge. Likewise, the concept of patient safety extends to the system environment and throughout its operational interdependency of care. Effective safety interventions must consider both perspectives.
This project goes on to identify that error largely occurs within the interaction between people and the systems in which they work. Patient safety is a property of system design, to make risky interventions reliably safe. System design may include materials, procedures, environment, training, and the culture.
Human factors are one consideration when designing safe systems. Human factors connect human performance to the environment. This considers how people work and constructs systems and products to encourage proper performance (WHO, 2007b; Gosbee, 2010; Emanuel et al., 2008). These designs include:
- Building redundancy into the process
- Creating forcing functions
- Reducing steps to simplify the process
- Self-explanatory controls
- Minimizing reliance on memory
- Standardizing common processes
- Decreasing reliance on vigilance (Gosbee, 2010; Emanuel et al., 2008).
Regardless of the aspect of patient safety being considered, some degree of education is likely required before full implementation can be realized. Therefore, understanding how best to educate staff is just as important as the safety concept itself.
The Higher Domains of Learning and the Adult Learner
In 1956, Benjamin Bloom led a group of educators to develop a classification of thinking behaviors important to the learning process. Eventually this became a taxonomy of six cognitive levels of complexity that was revised slightly in the 1990s (Table 2).
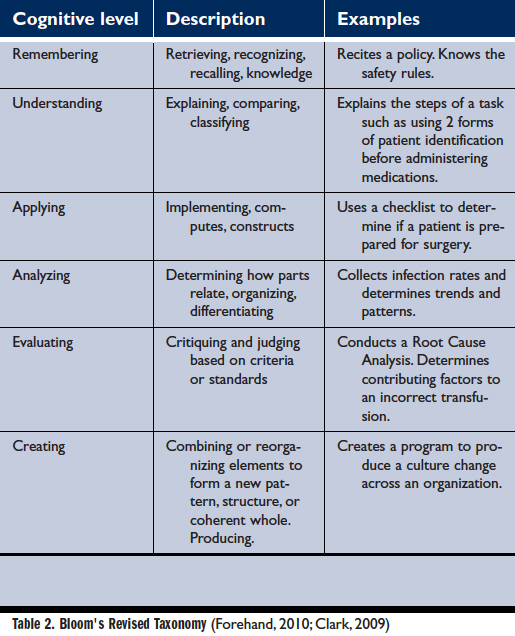
From the basic Remembering to the highest level of Creating, Bloom’s Revised Taxonomy shows how information is processed more comprehensively through progressively higher domains of learning, requiring more active participation by the learner. As an example, few would agree that memorization of fact translates into a meaningful change of behavior anymore than the ability to recite the alphabet implies the leaner can apply that knowledge to read, write, or evaluate the content of a book. In keeping with this concept, the transfer of newly acquired learning to a different situation must be viewed as fundamental to a successful learning experience (Thomas, 2007).
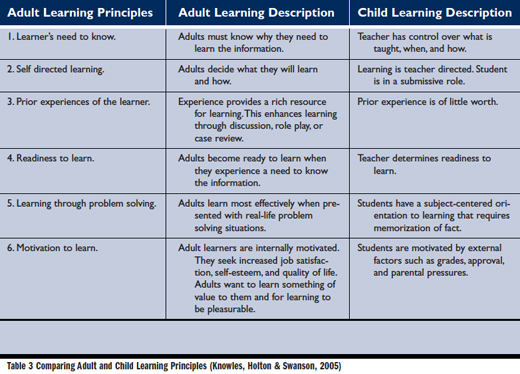
Additionally, adults have unique characteristics in terms of learning. As Table 3 shows, the motivations for adult learners are quite different from their younger counterparts. Unlike school-aged children, adults prefer to be in control their own learning. This may be a difficult concept for instructors to accept. From assisting with developing objectives, to the desire for feedback pertaining to their accomplishments, and opportunity for self-reflection, adults want to be consulted (Kaufman, 2003; Emanuel et al., 2008).
For example, conducting a needs assessment can be accomplished at the beginning of the instruction by asking relevant questions such as, “Do you know of a situation when a patient was incorrectly identified?” Asking for input regarding goals and learning methods helps establish the value of the learning experience for the adult learner (Knowles, Holton, & Swanson, 2005).
Being self-directed, adults seek new processes and information relevant to their individual life. They want to learn more about what to do and how to do it rather than general theory. Perhaps most importantly, adults are problem-oriented learners and prefer real-life examples of dilemmas to resolve. This also must utilize and acknowledge the wide range of experiences, skills, and knowledge adults bring to the learning environment (Kaufman, 2003).
By utilizing adult learning principles and Bloom’s Revised Taxonomy cognitive domains of learning, a challenging problem-solving learning environment can be established to maximize the potential to identify and integrate safety processes into routine practice. This creates the opportunity for the application of newly acquired information and skills into a range of situations found in healthcare (Thomas, 2007). The potential of this methodology to protect patients from harm is apparent.
Applying Adult Learning to Patient Safety Situations
The classroom setting for adults is also unlike that for children. For learning to occur, adults require a high degree of interaction. Therefore, instruction should:
- Build on existing knowledge and establish an association with the new information.
- Anchor all learning to a larger problem.
- Encourage learner ownership of the problem or task.
- Teach an authentic task without extraneous material.
- Present practical, relevant material that integrates into practice.
- Provide a realistic and challenging environment for the new learning to be practiced and applied.
- Encourage testing of ideas against alternative views.
- Allow opportunity for self-reflection on the learned content (Kaufman, 2003; Knowles, Holton, & Swanson, 2005).
Active learning that is analyzed, discussed, linked to relevant activity, incorporated into decision-making processes, or challenged with a problem is retained approximately three times better than lecture-based learning. It is also more likely to be integrated into practice (Emanuel et al., 2008).
Therefore, learning within realistic scenarios with complex situations requiring cognitively active skills listed on Bloom’s Revised Taxonomy (such as applying, analyzing, evaluating, and creating), has diverse application in patient safety concerns.
Table 4 provides examples of problem-oriented challenges pertinent to patient safety and lists the associated learning considerations including safety environment and human factors. The intent is to create interactive situations supportive of adult learning characteristics while broadening an appreciation for preventing harm.
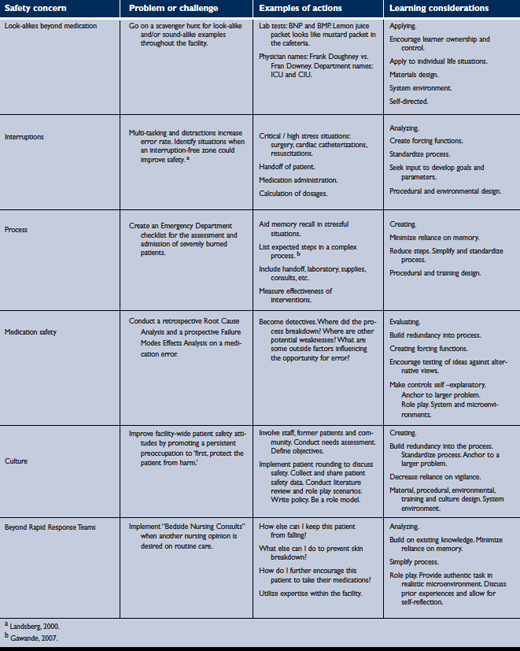
(click here to view a larger version in a separate window)
Realistic problem-solving builds on existing knowledge and skills to integrate newly acquired learning into safe practice. This form of instruction is ideal for small group settings as it allows for in-depth exploration of issues while encouraging critical thinking and teamwork. Problem-solving scenarios also address adult learning principles of self-directed learning and offer opportunities for self-reflection and evaluation (Emanuel et al., 2008).
Within adult learning environments, instructors assume a facilitator role rather than that of a lecturer or teacher. A facilitator is less a transmitter of knowledge than a guide to learning (Kaufman, 2003). Facilitators allow learners to experience learning on their own terms by steering learners toward analyzing, critiquing, and assessing new information or the problem to be solved. It is essential to create a comfortable climate of mutual respect to encourage the testing and sharing of new ideas (Knowles, Holton, & Swanson, 2005). The environment must be a non-threatening one where the learner’s experience counts as much as the facilitator’s knowledge. This allows adult learners and the facilitator to share information and perspectives as equals.
Conclusion
Patient safety aligns with the medical professional imperative of the Hippocratic oath to “First, do no harm.” It is ironic that healthcare has become a casualty of its own success to save lives. As rapid advances have overwhelmed long-established processes and systems, healthcare has produced tragic statistics in regard to medical error.
Despite a decade of data showing the prevalence of patient harm and the resulting financial disincentives, litigation associated with medical error, and educational attempts to prevent re-occurrence, there is little evidence of improvement in patient safety.
Education however, is one variable over which we have direct control. A highly interactive and problem-based approach is required to promote in-depth learning and application of new information. By utilizing multiple elements of instructional methods unique to adult learners, education has the potential to promote the attitudes and behaviors necessary to reduce patient harm (Emanuel et al., 2008).
According to B. F. Skinner, “Education is what survives when what has been learned has been forgotten” (The Quotations Page, 2010). The cognitive level of remembering and knowledge is not sufficient to establish and maintain behavior change within a dynamic system. As there will be more advances in healthcare and with them, new ways to harm patients, higher levels of cognition are required to enable healthcare workers to analyze patient safety concerns and pro-actively intervene at the bedside and across an ever-changing healthcare system.
Without a doubt, compassionate people have sworn to uphold the oath to first, do no harm. In view of increasing complexity and the abundance of change and medical error within healthcare, a renewed passion to a more pro-active pledge is in order. First, protect the patient from harm. Through effective, highly interactive education targeted to the needs of adults lies this essential and fundamental directive to improve the safety of patients everywhere.
Barbara Duffy is performance improvement and patient safety manager at Florida Hospital Memorial Medical Center in Daytona Beach, Florida. She may be contacted at duffyb@cfl.rr.com.